
Medical information note
This resource is for general education only and is not a substitute for medical advice, diagnosis, or treatment. Talk with a qualified clinician about severe symptoms, breathing problems, medication questions, symptoms in a child, or concerns about your personal health history.
Why Raw Fruit Can Make Your Mouth Itch
You bite into a fresh apple, peach, melon, or carrot and within minutes your lips tingle, the roof of your mouth itches, or your throat feels scratchy. The same food may cause no problem when it is baked, canned, or cooked.
That pattern can point to Pollen Food Allergy Syndrome (PFAS), also called Oral Allergy Syndrome (OAS). It happens when a person with pollen allergy reacts to similar proteins in certain plant foods. The immune system recognizes the food protein as if it were the pollen allergen and releases histamine at the point of contact, usually in the lips, mouth, tongue, or throat.
Quick answer: PFAS is an IgE-mediated food allergy caused by cross-reactivity between pollen and structurally similar proteins in raw fruits, vegetables, herbs, spices, seeds, peanuts, or tree nuts. Most reactions remain localized to the mouth, but throat symptoms, reactions beyond the mouth, reactions to cooked forms, and peanut or tree-nut reactions require greater caution.
PFAS is not the same as food intolerance, oral irritation from acidic foods, or a classic primary food allergy. The overlap can be confusing, so the safest diagnosis combines your symptom history, pollen pattern, food preparation, and allergist-directed testing.
PFAS at a Glance
| Question | Typical PFAS pattern | Reason to seek prompt medical advice |
|---|---|---|
| What triggers it? | A raw plant food linked to a pollen allergy. | Peanut, tree nuts, cooked foods, or an unclear trigger. |
| Where are symptoms? | Lips, tongue, mouth, ears, or mild throat itch. | Widespread hives, facial swelling, breathing symptoms, vomiting, dizziness, or fainting. |
| How fast does it start? | Usually within minutes of eating. | A reaction that is rapidly intensifying or affecting multiple body systems. |
| Does cooking help? | Often, because many cross-reactive proteins are heat-labile. | A reaction to cooked, baked, canned, or pasteurized forms. |
| Is it seasonal? | It can occur year-round but may worsen during the related pollen season. | Symptoms are becoming progressively stronger or occurring with smaller amounts. |
| What should you avoid? | The specific raw food that causes symptoms. | Do not create a broad elimination diet without clinical guidance. |
What Is Oral Allergy Syndrome?
PFAS is a type I, IgE-mediated hypersensitivity reaction. In many cases, pollen sensitization develops first. The immune system produces IgE antibodies to a pollen protein, then those antibodies recognize a similar protein in food.
For example:
- Birch pollen proteins can resemble proteins in apple, pear, peach, cherry, carrot, celery, and hazelnut.
- Grass pollen proteins can resemble proteins in melon, tomato, orange, peach, and celery.
- Ragweed pollen proteins can resemble proteins in banana, melon, cucumber, zucchini, chamomile, and sunflower seed.
- Mugwort pollen can cross-react with celery, carrot, parsley, coriander, fennel, anise, and caraway.
The term oral allergy syndrome describes the common mouth-focused symptoms. Pollen Food Allergy Syndrome is the broader and more clinically precise name because reactions are not always limited to the mouth.
Why PFAS is usually localized
Many proteins involved in PFAS, including PR-10 proteins and profilins, are unstable. Heat and digestion often change their shape quickly. That limits how much intact allergen reaches the bloodstream, which is one reason most reactions remain around the mouth and throat.
That reassuring pattern is common, but it is not universal. Different protein families have different heat and digestion stability. A reaction to peanut, tree nuts, cooked foods, or symptoms beyond the mouth should not be dismissed as routine PFAS.
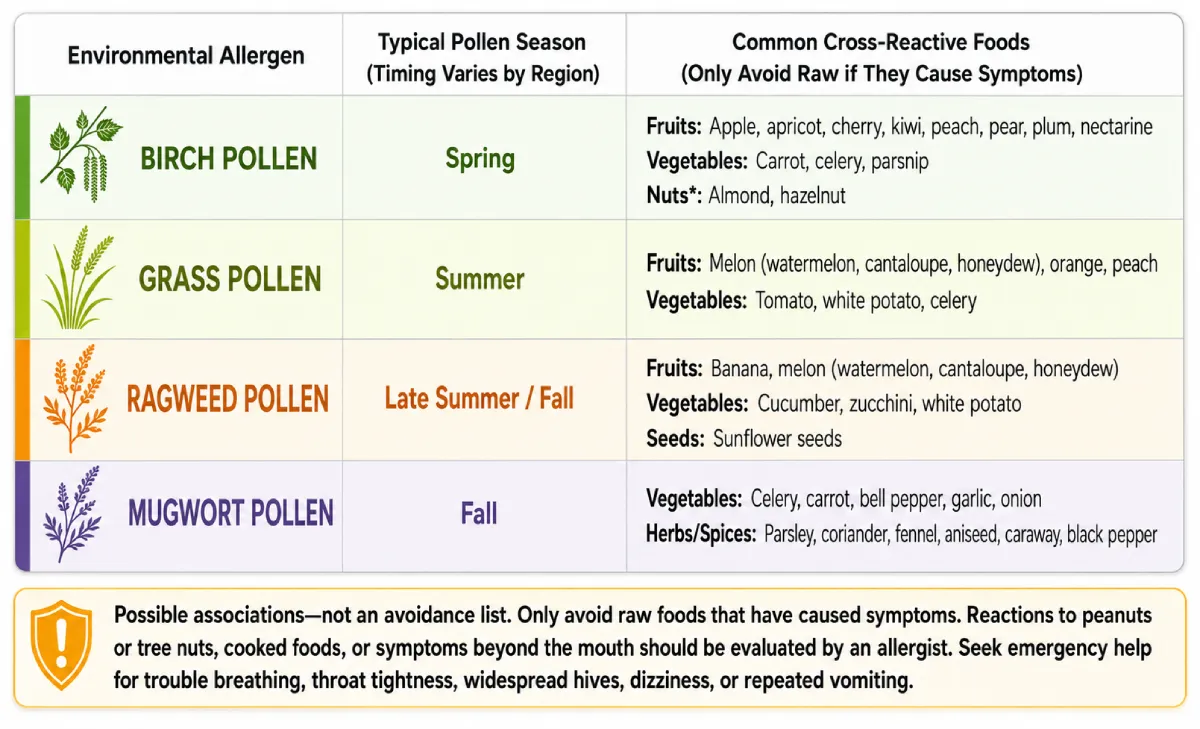
The Pollen-Food Cross-Reactivity Chart
Use this chart to identify possible links between a known pollen allergy and raw foods. It is a starting point, not an automatic avoid list. Many people with pollen allergy tolerate every food shown, and a person may react to only one food in a category.
Accessible chart summary
| Pollen group | Typical peak | Raw foods commonly associated with PFAS |
|---|---|---|
| Birch | Spring | Apple, pear, peach, plum, cherry, apricot, nectarine, kiwi, carrot, celery, parsnip, potato, hazelnut, almond, and sometimes other tree nuts. |
| Grass | Late spring and summer | Melons, orange, peach, tomato, celery, and potato. |
| Ragweed | Late summer and fall | Banana, watermelon, cantaloupe, honeydew, cucumber, zucchini, sunflower seed, and chamomile. |
| Mugwort | Late summer and fall | Carrot, celery, parsley, coriander, fennel, anise, and caraway. |
The list is not exhaustive. Cross-reactivity differs by region, pollen exposure, plant variety, protein family, and the individual person's immune response.
To compare the timing of the major pollen groups, see Tree Pollen vs. Grass Pollen vs. Weed Pollen.
Is pollen high in your area today?
Check your local forecast and plan your day around pollen levels.
Birch Pollen and Raw-Food Reactions
Birch-related PFAS is one of the best-known patterns. The main birch allergen, often referred to as Bet v 1, has structurally similar proteins in many fruits, vegetables, and nuts.
Common birch-associated foods
- Apple and pear.
- Peach, cherry, plum, apricot, and nectarine.
- Kiwi.
- Carrot, celery, parsnip, parsley, and potato.
- Hazelnut and almond.
- Soy in some people.
A person may tolerate one apple variety but react to another. Ripeness, storage, peeling, preparation, and pollen season can also change symptom intensity.
Why nuts deserve extra caution
Mouth itching from hazelnut or almond can fit a birch-related PFAS pattern, but it can also overlap with a primary tree-nut allergy. The same caution applies to peanut. Because primary peanut and tree-nut allergies can cause severe systemic reactions, do not rely on a food chart or cooking experiment to decide that a nut reaction is harmless.
Stop eating the suspected nut and arrange an allergist evaluation, especially if you have throat discomfort, hives, vomiting, breathing symptoms, dizziness, or a reaction to roasted or processed forms.
Grass Pollen and Raw-Food Reactions
Grass-associated PFAS is often linked with:
- Watermelon, cantaloupe, and honeydew.
- Tomato.
- Orange.
- Peach.
- Celery.
- Potato.
These links are possibilities rather than rules. A high grass pollen count does not mean you need to avoid tomatoes or melons. The clinically relevant food is the one that repeatedly causes symptoms.
If grass season brings nasal allergies and the same period brings mouth itching from raw produce, document both patterns. That history can help an allergist choose focused testing rather than ordering a broad, low-value food panel.
Ragweed Pollen and Raw-Food Reactions
Ragweed-related PFAS often appears in late summer or fall, although food reactions can happen at any time of year.
Common associations include:
- Banana.
- Watermelon, cantaloupe, and honeydew.
- Cucumber.
- Zucchini.
- Sunflower seed.
- Chamomile.
A person with ragweed allergy may notice stronger reactions during peak ragweed season. Track the food, portion, preparation, symptom timing, and local pollen level rather than assuming every melon or squash must be removed.
For a deeper look at ragweed season, symptoms, and treatment, read the Ragweed Allergy Guide.
Mugwort, Celery, and Spice Cross-Reactivity
Mugwort-associated PFAS can involve a celery-spice pattern. Possible triggers include:
- Celery.
- Carrot.
- Parsley.
- Coriander or cilantro.
- Fennel.
- Anise.
- Caraway.
Spice blends can make the trigger difficult to identify because labels may use collective terms such as “spices” or because a meal contains several botanically related ingredients. Bring ingredient lists, restaurant details, and photos of packaging to your appointment when possible.
Celery can be an exception to the simple “cooking makes PFAS safe” rule. Relevant proteins may remain clinically important after preparation in some people, so a cooked celery reaction deserves specialist evaluation.
Expected PFAS Symptoms vs. Red Flags
Most PFAS reactions are mild, immediate, and limited to the area that touched the food. However, “usually mild” should never be interpreted as “incapable of becoming serious.”
Symptoms that fit a typical localized pattern
- Itching or tingling of the lips.
- Itching of the tongue or roof of the mouth.
- A scratchy sensation in the throat without tightness or breathing difficulty.
- Mild lip or tongue swelling.
- Itchy ears.
- Small contact hives around the mouth.
- Symptoms beginning within minutes of eating the raw food.
- Symptoms settling after the food is removed or swallowed.
Stop eating the food when symptoms begin. Rinse your mouth and follow the plan provided by your clinician. Do not continue eating to “test” whether the reaction will stay mild.
Red flags that require urgent action
Emergency warning: Use prescribed epinephrine immediately according to your action plan and call 911 for breathing difficulty, wheezing, throat tightness or closure, hoarseness, fainting, collapse, blue or gray skin, or a rapidly worsening reaction. Antihistamines and asthma inhalers are not substitutes for epinephrine in anaphylaxis.
Seek urgent medical care for:
- Difficulty breathing, wheezing, persistent coughing, or chest tightness.
- A feeling that the throat is closing.
- Hoarseness, trouble speaking, or trouble swallowing saliva.
- Swelling that is rapidly increasing.
- Hives or swelling away from the mouth.
- Repeated vomiting, severe cramping, or diarrhea with other allergic symptoms.
- Dizziness, confusion, weakness, fainting, or a weak pulse.
- Pale, blue, or gray lips or skin.
- Symptoms involving more than one body system.
- A reaction that is escalating quickly, even if it started with mouth itching.
ACAAI cites research in which nearly 9% of PFAS patients developed systemic symptoms and 1.7% developed anaphylactic shock. Those figures should not be used to predict an individual's risk, but they reinforce why symptoms beyond the mouth need a medical plan.
Five Patterns That Need an Allergist, Not a Home Experiment
Arrange specialist evaluation if any of the following apply:
- Peanut or tree nuts cause mouth or throat symptoms. This may be PFAS, primary nut allergy, or both.
- Cooked food causes a reaction. Heat-stable allergens may be involved.
- Symptoms move beyond the mouth. Hives, vomiting, cough, wheeze, dizziness, or faintness are not a routine localized pattern.
- Throat symptoms are significant or worsening. Trouble swallowing, voice change, tightness, or closure needs urgent assessment.
- The amount needed to trigger symptoms is decreasing. Increasing sensitivity or changing reactions should be reviewed.
Also seek advice if reactions occur during exercise, after alcohol, or around use of nonsteroidal anti-inflammatory drugs such as ibuprofen. These can act as cofactors in some food reactions and may change severity.
How PFAS Is Diagnosed
PFAS is a clinical diagnosis. The most useful evidence is a repeatable connection between:
- An established or suspected pollen allergy.
- Immediate symptoms after a particular raw plant food.
- Better tolerance of a cooked or processed form, when applicable.
- A seasonal pattern that matches the related pollen.
An allergist may use:
- Skin prick testing to relevant pollens and selected foods.
- Specific IgE blood testing when skin testing is not suitable or when additional information is needed.
- Prick-to-prick testing with fresh food, because commercial food extracts do not always contain the unstable proteins responsible for PFAS.
- Component-resolved testing in selected peanut or tree-nut cases to help distinguish pollen-related sensitization from proteins associated with primary food allergy.
- A supervised oral food challenge when the history and tests do not provide a clear answer.
A positive test alone does not prove clinical allergy. Testing must match what happens when you eat the food. Broad food panels can produce sensitization results that lead to unnecessary avoidance.
Review the testing process in Allergy Testing: Skin Prick vs. Blood Test.
How to Build a Safer Food Plan
1. Avoid the raw food that caused the reaction
Current expert consensus supports avoiding the specific raw food responsible for your reaction, not every theoretically cross-reactive food on a chart.
That means a birch-allergic person who reacts to raw apple but tolerates pear, carrot, cherry, and hazelnut does not automatically need to remove all of them.
2. Do not use the chart as a challenge list
A cross-reactivity chart is not an invitation to test foods at home. Do not deliberately try a food that has caused throat symptoms, systemic symptoms, or a nut reaction. Ask an allergist whether testing or a supervised challenge is appropriate.
3. Cooking may help, but it is not a guarantee
Heating often changes PFAS proteins enough to prevent a reaction. Depending on the food and your history, you may tolerate:
- Baked fruit.
- Cooked vegetables.
- Microwaved foods.
- Canned fruit or vegetables.
- Pasteurized juice.
Use caution:
- Never assume peanut butter or roasted nuts are safe because raw nuts caused only mouth itching.
- Do not try a cooked form at home after breathing symptoms, widespread hives, vomiting, dizziness, or significant throat symptoms.
- Reactions to cooked foods may point to more stable allergens and deserve specialist assessment.
- Heating does not make every allergen harmless.
4. Peeling may reduce exposure for some fruits
Some cross-reactive proteins are concentrated near a fruit's skin, so peeling can lessen symptoms for some people. It is an optional comfort strategy for a previously mild, localized reaction—not a safety guarantee.
5. Keep a food-reaction record
Record:
| Detail | What to write down |
|---|---|
| Food | Exact food and variety, such as Gala apple or raw carrot. |
| Preparation | Raw, peeled, baked, canned, frozen, dried, blended, or cooked. |
| Amount | One bite, half a fruit, full serving, or unknown. |
| Timing | Minutes between eating and the first symptom. |
| Symptoms | Mouth itch, throat scratch, swelling, hives, cough, vomiting, dizziness, or other signs. |
| Duration | How long symptoms lasted and whether they worsened. |
| Treatment | Food stopped, mouth rinsed, antihistamine, epinephrine, or emergency care. |
| Context | Exercise, alcohol, illness, medication, pollen season, restaurant meal, or mixed dish. |
This record is often more useful than trying to remember a reaction months later.
Antihistamines, Epinephrine, and Emergency Planning
A clinician may recommend an oral antihistamine for limited itching, but antihistamines do not stop airway swelling, shock, or anaphylaxis. They should never delay epinephrine when severe symptoms are present.
An allergist may recommend carrying epinephrine if you have:
- Experienced symptoms beyond the mouth.
- Had significant throat discomfort or trouble swallowing.
- Reacted to a cooked form.
- Reacted to peanut, tree nuts, or another higher-risk food.
- Had a previous severe reaction.
- Asthma or other factors that may increase risk.
If epinephrine is prescribed:
- Carry it as directed.
- Know how and when to use it.
- Check the expiration date.
- Store it according to product instructions.
- Make sure family, school, workplace, or caregivers understand the plan.
- Follow the emergency action plan after use.
Can Allergy Shots or Sublingual Immunotherapy Treat PFAS?
Allergen immunotherapy can be effective for the underlying pollen allergy, but its benefit for PFAS is inconsistent. Some patients report improvement in food symptoms after pollen allergy shots; others do not.
Current expert consensus is clear on the main point: PFAS by itself should not be the primary reason to start pollen immunotherapy. The decision should be based on the severity of allergic rhinitis or asthma, confirmed pollen sensitization, exposure, treatment response, and the overall benefits and risks.
Do not attempt “desensitization” by eating progressively larger amounts of a trigger food without a specialist-supervised protocol. Experimental approaches involving structured food exposure are not the same as casually increasing portions at home.
For the standard allergy-shot process, see Allergy Shots: What to Expect, Timeline, Benefits, and Risks.
PFAS vs. Primary Food Allergy
The distinction matters because the expected risk and management can differ.
| Feature | PFAS pattern | Primary food allergy pattern |
|---|---|---|
| Underlying sensitization | Usually begins with pollen allergy. | Begins with sensitization to proteins in the food itself. |
| Common foods | Raw fruits, vegetables, herbs, spices, some nuts, peanut, or seeds. | Any food; common examples include peanut, tree nuts, milk, egg, wheat, soy, fish, shellfish, and sesame. |
| Preparation | Cooked forms are often tolerated, but not always. | Reactions may occur to raw and cooked forms. |
| Typical symptoms | Immediate mouth and throat itching or mild localized swelling. | Skin, breathing, gastrointestinal, cardiovascular, or multi-system symptoms may occur. |
| Severity | Usually mild and localized, with rare systemic reactions. | Can range from mild to life-threatening. |
| Testing | History plus pollen and targeted food evaluation. | History plus targeted testing; oral challenge may be needed. |
A person can have both PFAS and a primary food allergy. That is why peanut and tree-nut symptoms require careful interpretation rather than reassurance based on pollen allergy alone.
When Symptoms Are Not PFAS
Mouth discomfort after food has other possible explanations, including:
- Acidic irritation from citrus, tomato, or pineapple.
- Spicy-food irritation.
- Contact irritation from cinnamon or flavorings.
- Burning mouth syndrome.
- Oral thrush or another infection.
- Reflux.
- Dental or gum disease.
- A primary food allergy.
- Food intolerance, which usually causes digestive symptoms rather than immediate mouth itching.
- Latex-fruit cross-reactivity.
Seek medical evaluation when the pattern is unclear, symptoms persist without eating, the mouth has sores or visible changes, swallowing is difficult, weight loss occurs, or symptoms are not limited to raw plant foods.
Questions to Ask an Allergist
Bring your reaction log and ask:
- Does my history fit PFAS, a primary food allergy, or both?
- Which pollen sensitization best explains my food reactions?
- Should I have skin testing, specific IgE testing, component testing, or a supervised food challenge?
- Are reactions to this peanut or tree nut considered higher risk?
- Is it safe for me to try a cooked, peeled, or canned form?
- Which foods should I avoid, and which tolerated foods should remain in my diet?
- Do I need an epinephrine prescription and written action plan?
- Could exercise, alcohol, medication, illness, or pollen season be making reactions worse?
- Would pollen immunotherapy be appropriate for my nasal allergy or asthma, independent of PFAS?
To locate a specialist who can distinguish PFAS from primary food allergy, use the AllergyAva allergist directory.
Final Takeaway
Oral Allergy Syndrome is a real IgE-mediated food allergy, but it behaves differently from many primary food allergies. A repeatable itchy-mouth reaction to a raw fruit or vegetable, especially when the cooked version is tolerated, strongly suggests a pollen-food cross-reaction.
Use the chart to recognize patterns—not to create a sweeping avoidance diet. Stop eating foods that cause symptoms, document the details, and seek allergist guidance for nut reactions, cooked-food reactions, significant throat symptoms, worsening reactions, or any symptom beyond the mouth.
Breathing difficulty, throat closure, hoarseness, widespread hives, repeated vomiting, dizziness, collapse, or rapidly worsening symptoms can indicate anaphylaxis. Use prescribed epinephrine immediately according to your emergency plan and call 911.
This content is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Do not perform a home food challenge after a significant reaction. Seek emergency care for severe, rapidly worsening, or multi-system allergic symptoms.
Frequently Asked Questions
Is oral allergy syndrome a true food allergy?
Yes. Pollen Food Allergy Syndrome is an IgE-mediated food allergy caused by cross-reactivity between pollen proteins and similar proteins in plant foods. It is often called a secondary food allergy because pollen sensitization usually comes first.
What does oral allergy syndrome feel like?
Typical symptoms include immediate itching, tingling, burning, or mild swelling of the lips, tongue, roof of the mouth, ears, or throat after eating a raw fruit, vegetable, or nut.
How quickly do PFAS symptoms start?
Symptoms usually begin within minutes of chewing or swallowing the trigger food, although delayed reactions can occasionally occur. Mild localized symptoms often settle soon after the food is removed or swallowed.
Can oral allergy syndrome cause anaphylaxis?
Yes, but severe systemic reactions are uncommon. Breathing difficulty, throat closure, widespread hives, repeated vomiting, dizziness, or fainting require immediate emergency treatment.
Should I avoid every food on the pollen food chart?
No. A chart lists possible cross-reactions, not foods that every pollen-allergic person must avoid. Avoid foods that cause symptoms and ask an allergist before making broad dietary restrictions.
Can cooking prevent oral allergy syndrome symptoms?
Often, because many PFAS proteins are damaged by heat. However, cooking is not a guarantee, especially for peanuts, tree nuts, celery, or anyone who has reacted to cooked food or had symptoms beyond the mouth.
Does peeling fruit prevent PFAS?
Peeling may reduce symptoms for some fruits because relevant proteins can be concentrated near the skin, but it is not a reliable safety measure after significant throat or systemic reactions.
Can children have oral allergy syndrome?
Yes. PFAS is more common in older children, teenagers, and adults who have already developed seasonal pollen allergy, but a qualified allergist can evaluate symptoms at any age.
Why are PFAS symptoms sometimes worse during pollen season?
Your immune system may be more reactive when the related pollen is abundant, so a raw food that causes little trouble at other times may trigger stronger mouth symptoms during that pollen season.
Can I eat peanut butter if raw peanuts make my mouth itch?
Do not assume peanut butter is safe. Peanut proteins can remain allergenic after roasting, and mouth or throat symptoms from peanut may represent primary peanut allergy rather than mild PFAS. Stop eating it and seek allergist evaluation.
Are tree nuts different from fruits and vegetables in PFAS?
Yes. Mouth itching from hazelnut, almond, walnut, or other nuts can overlap with PFAS but may also signal a primary nut allergy with greater anaphylaxis risk. An allergist should assess nut reactions.
How is pollen food allergy syndrome diagnosed?
Diagnosis is based mainly on the reaction history and pollen allergy pattern. An allergist may use skin testing, specific IgE blood testing, fresh-food prick-to-prick testing, or a supervised oral food challenge when needed.
Do allergy shots cure oral allergy syndrome?
Not reliably. Allergy shots may improve PFAS in some people while treating the underlying pollen allergy, but current expert consensus says PFAS alone should not be the main reason to start immunotherapy.
Should I carry epinephrine for oral allergy syndrome?
An allergist may recommend epinephrine if you have had symptoms beyond the mouth, significant throat symptoms, reactions to cooked foods, peanut or tree-nut reactions, or other risk factors for a severe reaction.
When should I call 911 after eating a PFAS trigger?
Call 911 for trouble breathing, wheezing, throat tightness or closure, hoarseness, faintness, collapse, blue or gray skin, rapidly spreading hives, or a rapidly worsening reaction. Use prescribed epinephrine immediately according to your emergency plan.
Sources
AllergyAva uses public health, clinical, data, and product documentation to support resource updates.
Oral Allergy Syndrome Symptoms Diagnosis and Treatment
AAAAI
View sourcePollen Food Allergy Syndrome
ACAAI
View sourceOral Allergy Syndrome Pollens and Cross-Reacting Foods Chart
AAAAI
View sourceInternational Delphi Consensus on Pollen-Food Allergy Syndrome Management
AAAAI and JACI In Practice
View sourceAnaphylaxis Emergency Action Plan
AAAAI
View sourceFood Allergy
AAAAI
View sourceBirch Pollen Immunotherapy and PFAS Research Summary
AAAAI
View source
Next steps
Turn allergy guidance into a local plan
Keep reading
Related AllergyAva resources
Understanding Pollen Allergies: Symptoms, Triggers, Pollen Season, Treatment, and Relief Guide for 2026
How to Prepare for Spring Allergy Season 2026: Expert Checklist
Editorial standards
Resources are prepared by the AllergyAva Editorial Team. Health-information pages are clinically reviewed before publication. Content is informational and is not a substitute for personal medical advice.
Read our review policy